
It is usually patients not doctors who balk at the sight of a medical instrument being unwrapped. But the flatus tube, used to treat a condition of the sigmoid colon, is one no surgeon relishes.
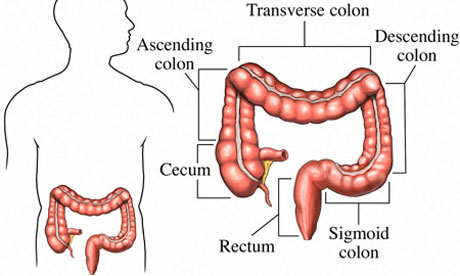
The sigmoid is an S-shaped stretch of large bowel, about 40cm long, which leads up to the rectum. Its main function is to store faeces until it is ready to enter the rectum and be expelled through the anus, and it is the site of a variety of problems.
Inflammatory bowel disease such as ulcerative colitis and Crohn's disease may occur here. Diverticulitis, in which little outpouchings of bowel form and become inflamed, is more common in the sigmoid than any other part of the bowel. Small growths called polyps, as well as cancers, also favour this site.
The good thing about investigating sigmoid disease is that this part of the colon isn't far from the outside world. It is easy to pass a rigid sigmoidoscope into the anus and get a decent view. For a more detailed look patients are sedated so that a flexible sigmoidoscope can be introduced, and biopsies can be taken through this. If necessary, it is possible to remove the entire part of the colon in a sigmoidectomy. Usually, the remaining colon can then be joined to the rectum.
But it is another condition that makes junior doctors quake in their surgical boots. Volvulus is when a part of the bowel twists on the tissue which attaches it to the abdominal wall, forming an obstruction and it is commoner here. Patients are usually over 50 and chronically constipated. In A&E, they describe abdominal pain and not having passed faeces or wind for days. Simple x-rays may show a sigmoid colon so distended that it extends all the way up to the chest-bone.
Although definitive treatment often involves surgery, it is the junior doctor's job to deal with the acute situation with the help of the dreaded flatus tube. The patient lies on their side and a sigmoidoscope is inserted gently into the back passage. The junior then has to slowly manoeuvre the hollow flatus tube through the sigmoidoscope and into the obstructed loop. The key is to make sure the other end is directed over a bucket and not one's shoes. The patient's sense of enormous relief when fluid, flatus and faeces are expelled into the bucket is in inverse proportion to the doctor's discomfort.
• Gabriel Weston is a surgeon and author of Direct Red: A Surgeon's Story
